
Clinical Trial Results Showing efficacy of Nighttime Biofeedback as a Tool for the Reduction of Habitual Bruxism Activity and Related TMJ/TMD Symptoms.
by Lee Weinstein, BSEE
January 1, 2013
Introduction
The National Institutes of Health estimates that 10.8 million people suffer from TMJ disorder (TMD, aka TMJD) in the United States, and 90% of those sufferers are women in child-bearing years. In a recent study done at Tufts involving 504 TMD patients, about 70% of patients self-reported that they attributed their TMD symptoms to bruxism (1). It has long been known that Bruxism is one of the main causes of TMD, but until the recent advent of wearable, quantitative EMG measurement equipment, it has been difficult to measure the correlation between various TMD symptoms and the quantity of bruxism that a patient exhibits. The advent of the first EMG measurement headband in 2001 made quantitative assessment of bruxism much easier and more economical.

Figure 1
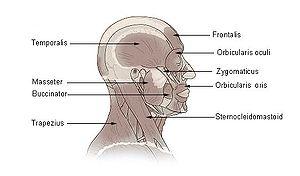
The EMG measurement and biofeedback headband used in this study uses conductive rubber pads that rest on the temples to pick up EMG signals from the temporalis muscles during sleep, and logs the number of clenching incidents, and the accumulated clenching time.
One of the most challenging things about bruxism to both patients and clinicians is that in many cases even if the initial cause of bruxism can be identified and eliminated, the bruxism behavior may have become habitual and thus the behavior may not be eliminated by the elimination of the cause. The habitual nature of bruxism is one of the reasons that all treatment modalities available prior to nighttime biofeedback (including splints, drugs, Botox, chiropractic techniques, acupuncture, etc.) have met with only limited success. In a survey of 300 habitual bruxers conducted through Google (2), no more than 15% of the patients that had used any one of these prior treatment modalities rated the modality highly effective.
There has been a large body of research to support the use of biofeedback to aid in treatment of TMD pain (3), with dental co-treatment (4-10), for temporomandibular joint (TMJ) muscle tension (11-15), and bruxism (16, 17). These studies were all done using tabletop biofeedback units that connect to the patient with wired adhesive electrodes. In this study we examine the efficacy of nighttime biofeedback in the reduction or elimination of habitual bruxism. Efficacy was measured through quantitative EMG measurements made during sleep, using the EMG measurement and biofeedback headband shown in figure 1. Although the majority of patients who participated in the study self-reported reduction or elimination of symptoms, the basis of this report is quantitative EMG measurements.
Therapeutic Intervention
The SleepGuard biofeedback headband (shown in figure 1) is an EMG measurement and biofeedback device worn on the head. It measures electromyographic signals (EMG) from the temporalis muscles. The headband may be used while awake or during sleep. In this study, patients wore the headband while sleeping. The headband can be worn either in silent mode (to measure baseline bruxism) or in biofeedback mode. In both modes it measures two things over the course of a night: a count of bruxism events, and the total accumulated clenching time of those bruxism events. The headband includes a piezoelectric tone generator which contacts the forehead and can produce an acoustic biofeedback tone which is heard through bone conduction in both ears.
When the headband is used in biofeedback mode, the tone starts at a low volume when clenching starts, and ramps up in volume after about one second if clenching continues. As soon as clenching stops, the tone stops. The intent is to provide a signal that patients can respond to (by relaxing their jaw muscles) in sleep, without waking up, thus cutting clenching incidents short and thus reducing the damage caused by clenching. In this study, the headband was worn by each patient for 30 nights. The first three nights, the headband was used at night in silent mode to gather baseline data. During this time the patients did a few minutes of wakeful practice responding to the tone, to increase their likely ability to respond in sleep. During the remaining 27 nights, the headband was used in biofeedback mode.
Clinical Trial Results
The first round of clinical trials to test the efficacy of using a biofeedback headband to reduce bruxism involved 92 patients. The total clenching time recorded by the biofeedback headband each night was logged on a daily basis. The first three days of data for each participant were baseline data. The remaining 27 days of data was data taken with the biofeedback turned on. Running the data through a statistical analysis package yielded a p value for the data of 10-16.
One illuminating way to view the data is to divide the clinical trial patients into four groups (quartiles), ranked by overall end reduction in nightly bruxism at the end of the trial versus the beginning. The four graphs below represent efficacy quartiles (23 patients each, with each graph representing the average of the normalized data from the 23 patients in the quartile). The most responsive quartile is shown first and the least responsive quartile is shown last. Average nightly reduction in bruxism time was measured as the difference between the normalized average nightly clenching time during the three days of initial baseline measurement (this average was normalized to 1 for all patients), and the normalized average nightly clenching time during the last three days of the trial.
The best performing quartile (23 patients) results are shown in figure 2 below.

Figure 2
Clenching time reduction of most efficacious quartile during 30-day clinical trial.
These patients showed an average initial reduction in bruxism time of 80% in one day after turning on the biofeedback, and by the end of the month they had a nightly bruxism time reduction of 90%. Since clenching force typically ramps up during a clench, cutting the clench short cuts out the most damaging part of the clench.
Since the body’s nervous system senses mostly differences and rates of change rather than absolutes, a clencher’s brain gets more of the clenching sensation it is addicted to by increasing bite force throughout each clench, and this is indeed what happens during a typical clench. The force-vs.-time diagram of a typical clench whose force linearly increases through the clench is shown in figure 3. The peak clenching force varies from person to person, as does the length of the clench, but the numbers shown in figure 3 are not uncommon.
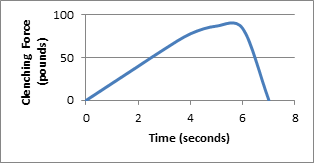
Figure 3
Typical variation of clenching force during a single Clench of a bad bruxer.
Assuming increasing clench force throughout a typical clench, and taking into account the probable average reduction of peak clenching force of 50% to 90%, gives a probable 95% to 99% reduction in nightly damage. Most patients in this quartile report substantial reduction or complete elimination of pain such as jaw pain, migraines, TMJ pain, etc..
The next best performing quartile (23 patients) is shown in figure 4 below.
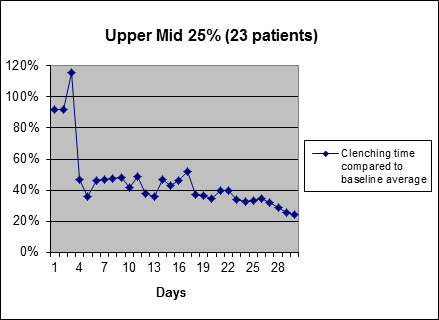
Figure 4
Clenching time reduction of second most efficacious quartile during 30-day clinical trial.
The "remaining bruxism" of these patients is about twice the most efficacious group (in terms of remaining clenching time), but still very low. Again, because the damaging, higher-force later part of each clench is not happening, the reduction in ongoing damage and pain may be reduced far more than one might think from the percentage reduction in clenching time indicated above.
As can be seen in both of the upper quartiles above, nightly clenching time was trending down steadily toward the end of the month, perhaps indicating that these patients are on the average training themselves out of their bruxism habit. This theory is supported by anecdotal evidence in follow-up interviews several months later, where a number of patients said that after using the biofeedback for between two and four months, they were able to go for long periods (over a month) without using the headband before any daily pain returned.
Most patients in the second quartile, like the first quartile, report substantial reduction or complete elimination of pain such as jaw pain, migraines, TMJ pain, etc..
The average of the data from the lower mid quartile (23 patients) is shown in figure 5 below.
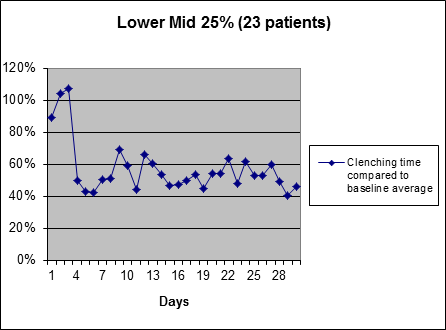
Figure 5
Clenching time reduction of third most efficacious quartile during 30-day clinical trial.
These patients experience approximately a 60% initial reduction in nightly clenching time when the biofeedback is turned on, and their nightly clenching times remain at roughly this level for the rest of the month. In addition to the reduction in clenching time, it is estimated that this group experiences a reduction in clenching force of about 50%.
There is no obvious trending downward toward the end of the month for this group, so there is no evidence that they are training themselves out of their bruxism habit, but continued use of the biofeedback appears to be a viable tool in ongoing mitigation of bruxism damage and pain. Some patients in this quartile reported a complete elimination of pain symptoms, including TMJ pain and migraines.
The data from the lowest-performing quartile (excluding one outlier, whose data is included in the whole group average, but whose data warps the average of the quartile significantly) is shown in figure 6 below.
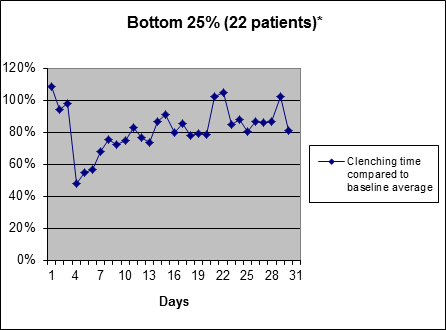
Figure 6
Clenching time reduction of least efficacious quartile during 30-day clinical trial.
These patients respond well to the biofeedback at first, and then over time, their nightly bruxism times came back to a level close to their baseline levels.
One way to interpret why this may happen is that each person may be thought of as being of "two minds". One part of the mind wants to learn to relax and get out of the bruxism habit. This part of the mind hears the biofeedback tone as a caring reminder about something important. The other part of the mind wants to learn to ignore any sound heard during sleep, and continue with any addictive behavior. For this group, this second part of the mind appears to win out, and patients return to near-baseline levels of clenching (though there is some reduction in clenching time and some reduction in clenching force, so they still benefit). This is discussed further in the later section titled “Efficacy Factors”.
Averaging the data from all 92 patients in the clinical trial, the overall average clenching time graph is shown in figure 7 below.
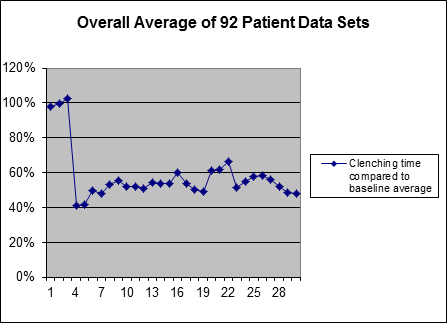
Figure 7
Average clenching time reduction of all 92 patients in clinical trial.
As can be seen by comparing the "overall average" graph above to the four quartile graphs, the overall average is only representative of a small percentage of people in the trial.
Discussion
To place the results of this study in proper context it is important to understand the neurological nature of habit formation and habit modification and their relationship to biofeedback and bruxism. Below we will first present a modern neurological model of habit formation and modification, which form the basis for the design of this study. After that premise is shared, we will discuss other treatments and how they fit within this neurological model of habit formation and modification. We will then present key differences between nighttime biofeedback and daytime biofeedback in the treatment of nighttime bruxism.
The Habitual Nature of Bruxism
How nighttime clenching becomes a habit
Lets take a look at how we human beings build habits. One of the key functions of the neocortex (the part of the brain that makes humans different from animals) is the formation and execution of habits. Habits enable us to do many things subconsciously and simultaneously, while our conscious attention can only handle doing one or two things. Recent brain research (18) has shown that the basic function of the neocortex is to memorize, recognize, predict, and replay patterns. Habit formation and the triggering of habitual actions (such as stepping on the brake when the brake lights of a car in front of you go on) are subsets of these basic cortex functions of memorizing, recognizing, predicting, and replaying patterns.
We survive by building thousands of such "good" habits, all of which are triggered by associated feelings or situations. Once a recognition sequence (of a feeling or situation) and the appropriate response action sequence have been learned, that recognition and those responses can (and do) become subconscious, in that the recognition of circumstances and the acting out of the response both happen without us thinking about it. There are many such recognition and action sequences involved in being able to do something like play a sport, or drive a car. Once a given recognition neuron has been wired up to trigger an action sequence neuron, it takes substantial re-training to prevent that triggering from happening, or to mitigate the action once it has been initiated. The perception patterns we learn to recognize to trigger a motor sequence (habit) can include all our senses, plus emotional states, plus imagined situations and emotions.
When we learn a habit such as bruxism, both an action sequence (clenching), and the resulting sensation sequence are stored in our brains through repetition, in the form of strengthened neural connections, and later either imagining the sensation sequence or something associated with it (or experiencing an associated emotion) can trigger the action subconsciously.
As we first develop a habit where there is no initial tendency, the (non-conscious) neural pathway from sensation sequence to desired action sequence could be thought of as a meandering pathway (sequence of neurons that fire) through an un-cut jungle to a destination (an action).


For habits where there is an initial tendency, a jungle with a path through it may be a better initial analogy.
Each time a particular neural pathway gets used, it gets strengthened. This happens physically at the synapses between neurons. So as the habit gets more entrenched, that path through the jungle may begin to look more like a road (which is easier to go down than a path).


When the habit becomes still more entrenched, it may look more like a highway.
The structure of breaking a habit
If we have a habit (a neural highway toward a particular action sequence such as bruxism) and we want to stop using that highway for a while so it can become “overgrown with trees and look more like a jungle.” How might this be accomplished?
With habits like fingernail biting or thumb-sucking, the answer may seem obvious. A way to change the habit is to develop awareness of the onset of the behavior, and then substitute a different behavior. Repeated conscious intervention is the key to modifying any habit. But how can a habit be modified if it occurs during sleep?
The key to modifying a habit that occurs during sleep is to provide some level of conscious awareness of the onset of the habitual action, so the sleeping person can substitute a different action sequence. Nighttime biofeedback can provide a signal at the onset of an action but the challenge remains as to how to recognize and respond to such a signal when sleeping. Most parents will realize through their own experience that if they hear a sound in the house that could indicate his or her child is in danger, the parent will usually suddenly wake. This sudden waking happens when a subconscious process in the cortex recognizes (for instance) a sound sequence that could indicate a child is in danger. If a signal is recognized during sleep, this signal could be effectively used to change a habit particularly if it can occur without awakening the patient.
Bruxism Habit Formation
Let's take a look at the stages of habit formation as they relate to bruxism:
(1) Neurologically Intense Thought/Emotion (for instance stress, traumatic memory of car accident, allergic reaction to a food, or reaction to a drug)
Initial Action (Clenching and/or grinding of teeth)
(2) Action Sequence (in presence of thought/emotion) Clench with force ramping up, then stop
Nerve Sensation Sequence from teeth
(3) Thought/Emotion --- Predictive memory of sequence
Habitual Muscle/Sensation sequence
While in the beginning it may be an exceptional circumstance, such as a traumatic event, or a very stressful period of time, or a drug or nutritional situation that throws the patient's system into imbalance, and results in bruxism, once Bruxism becomes a habit, it only takes a subconscious memory to trigger the previously memorized bruxism action sequence in sleep. As the bruxism happens, neural associations are built between emotions, physical sensations, and muscle actions. Additionally, memories are formed of those emotional states and physical sensations, and later recalling of those memories can trigger the associated muscle action sequences.
Detecting and Interrupting Bruxism
What is much more common is for bruxism to occur in a way which is imbalanced between the right and left sides of the head. During normal chewing, food is shifted between the left and right sides of the mouth, and the brain automatically actuates jaw muscles on opposite sides of the head in a ratio that shifts with the shifting of the food being chewed. Most people are able to consciously selectively actuate the jaw muscles on either side of their head if so instructed. The biofeedback headband is designed to detect muscle groups on both sides of the head, in order not to offer the brain the opportunity to subconsciously addictively seek to produce the feeling of clenching on only one side of the head to avoid detection.
Efficacy Factors
Daytime Response Conditioning
Prior to this clinical trial, interviews were conducted with 100 patients who had used the headband for bruxism reduction for at least two months. Anecdotal reports from those interviews indicated that patients who spent wakeful time training themselves to relax when they heard the biofeedback tone, did better than patients who did not.
Within the clinical trial presented herein, written instructions directed all participants to spend at least a few minutes per day in the first few days doing “response training” to train themselves to relax cooperatively and immediately when the tone was heard. The instructions explained that the intent was for this training to carry over into sleep, and increase the patient's ability to respond (by relaxing his or her jaw) in sleep without waking when the biofeedback tone is heard. No verification was done to confirm that patients understood the importance of the daytime conditioning, and no patient interviews were conducted to determine to what extent each patient followed the instructions concerning daytime conditioning.
In the year following the clinical trial, experiments were conducted with numerous patients whose results were analogous to those in the least efficacious quartile of the clinical trial, and more effective daytime conditioning practices were developed.
Mental Alignment With the Process
Mental alignment with the process has been found to be one of the key factors influencing efficacy. Patients who describe themselves as feeling grateful for the audio reminder to relax their jaw muscles, tend to decrease their nighttime clenching faster and by a higher percentage than patients who do not describe themselves as feeling grateful for the reminder. Thus, the suggestion of practicing feeling grateful has also been added to the suggested daytime conditioning.
Louder Biofeedback Sound Helps Some Deep Sleepers
Subsequent to the clinical trial, some patients who considered themselves heavy sleepers and whose results were analogous to those in the least efficacious quartile of the clinical trial were given biofeedback headbands modified to supply the biofeedback sound through an earphone rather than the standard piezoelectric transducer which contacts the forehead. About 50% of those patients were able to get bruxism reduction analogous to that of the more efficacious quartiles using a louder biofeedback sound through the earphone.
Conclusion
This clinical trial showed that about 75% of patients are able to reduce their nightly clenching substantially through ongoing use of the biofeedback headband in its standard configuration. On the average, the bulk of the benefit in nightly clenching time reduction is realized from the day the biofeedback is turned on. Reduction in pain or elimination of pain usually follows within several days. About 25% of patients appear to remain at the initially-reduced level ongoing, and there are indications that about 50% of patients are able to continue to steadily reduce their nightly clenching times beyond the initial reduction. Future research will include a follow up trial that is 60 days long instead of 30 days long, and includes 3-day baseline measurements after 27 days and after 57 days, as well as at the beginning of the trial. Another clinical trial is being designed specifically as a migraine reduction study.
Next Steps - Partners Wanted
Holistic Technologies is interested in partnering with professionals, including Doctors, Dentists, Chiropractors, and Physical Therapists to learn even more from this clinical trial (through patient interviews), and publish journal articles based on this trial and future work. Please contact us if such a partnership would be of interest to you.
References:
- van der Meulen MJ, Ohrbach R, Aartman IH, Naeije M, Lobbezoo F (2010). Temporomandibular disorder patients' illness beliefs and self-efficacy related to bruxism. J Orofacial Pain 24 (4): 367-372.
- Holistic Technologies LLC - On-line bruxism survey (2010) through Google AdWords re people searching on terms including the word bruxism.
- Carlsson SG, Gale EN. Biofeedback in the treatment of long-term temporomandibular joint pain: an outcome study. Biofeedback Self Regul. 1977 Jun;2(2):161-71.
- Principato JJ, Barwell DR. Biofeedback training and relaxation exercises for treatment of temporomandibular joint dysfunction. Otolaryngology. 1978 Sep-Oct;86(5):ORL-766-9.
- Dahlström L, Carlsson SG. Treatment of mandibular dysfunction: the clinical usefulness of biofeedback in relation to splint therapy. J Oral Rehabil. 1984 May;11(3):277-84.
- Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain. 1999 Winter;13(1):29-37.
- Müller F. [Biofeedback as a part of the treatment of mandibular dysfunctions]. [Article in German] Dtsch Zahnarztl Z. 1989 Dec;44(12):938-41.
- Medlicott MS, Harris SR. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder. Phys Ther. 2006 Jul;86(7):955-73.
- Crider A, Glaros AG, Gevirtz RN. Efficacy of biofeedback-based treatments for temporomandibular disorders. Appl Psychophysiol Biofeedback. 2005 Dec;30(4):333-45.
- Turk DC, Zaki HS, Rudy TE. Effects of intraoral appliance and biofeedback/stress management alone and in combination in treating pain and depression in patients with temporomandibular disorders. J Prosthet Dent. 1993 Aug;70(2):158-64.
- Jadidi F. Castrillon E, Svensson P. Effect of conditioning electrical stimuli on temporalis electromyographic activity during sleep. Journal of Oral Rehabilitation. 2008;35(3):171-83.
- Peck CL, Kraft GH. Electromyographic biofeedback for pain related to muscle tension. A study of tension headache, back, and jaw pain. Arch Surg. 1977 Jul;112(7):889-95.
- Moss RA, Wedding D, Sanders SH. The comparative efficacy of relaxation training and masseter EMG feedback in the treatment of TMJ dysfunction. J Oral Rehabil. 1983 Jan;10(1):9-17.
- Sherman RA. Relationships between jaw pain and jaw muscle contraction level: underlying factors and treatment effectiveness. J Prosthet Dent. 1985 Jul;54(1):114-8.
- Principato JJ, Barwell DR. Biofeedback training and relaxation exercises for treatment of temporomandibular joint dysfunction. Otolaryngology. 1978 Sep-Oct;86(5):ORL-766-9.
- Pierce CJ, Gale EN. A Comparison of Different Treatments for Nocturnal Bruxism. J Dent Res 67(3):597-601, March, 1988.
- Foster PS. Use of the Calmset 3 biofeedback/relaxation system in the assessment and treatment of chronic nocturnal bruxism. Appl Psychophysiol Biofeedback. 2004 Jun;29(2):141-7.
- Hawkins J, Blakeslee S. On Intelligence. First Edition. Henry Holt and Company: New York, NY. 2004: 106-76.